On December 18, Liu et al, a Japanese group reported the discovery of an infectivity enhancing site on the SARS-Cov2 spike protein, which is located on the N-terminal domain (NTD). Antibodies derived from Covid patients that bind to this site increase the infectivity by 2-3 fold in cell culture experiments. Binding of an antibody to the NTD enhances the spike protein binding to the ACE2 receptor of the host cell. All covid infected patients within their sample had virus enhancing antibodies. However the quantity and the ratio of (bad) virus enhancing antibodies to (good) virus neutralizing antibodies varied significantly between patients.
https://www.biorxiv.org/content/10.1101/2020.12.18.423358v1
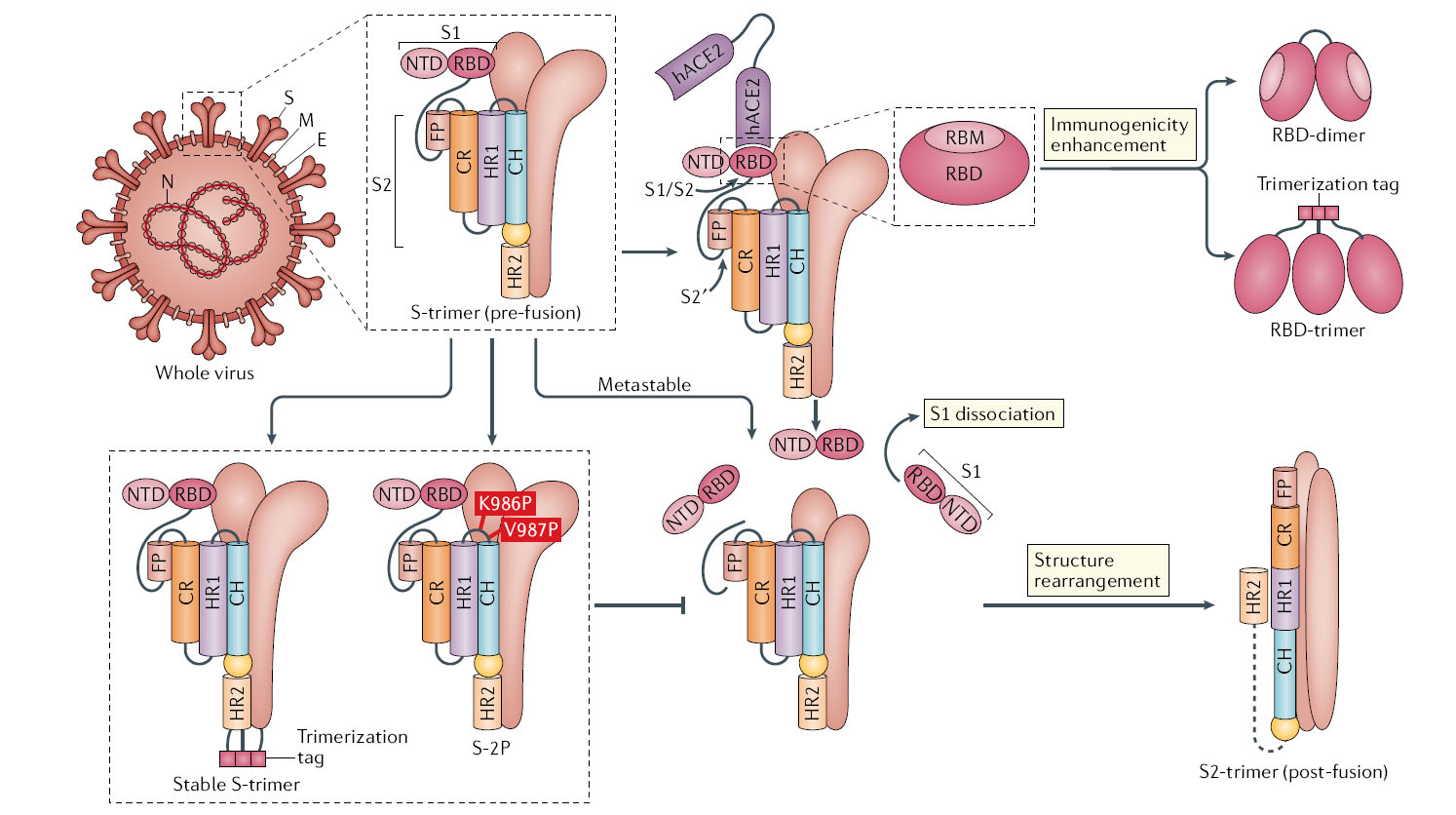
It should be noted that infectivity enhancing site is present on the modified spike protein used by the pfizer, moderna and astrazenecca vaccines as the immune target.
What is happening?
The spike protein is what used by the SARS-Cov2 virus to gain entry into a host cell. When the immune system is exposed to the SARS-Cov2 spike protein (by either vaccine or virus), it produces a variety of antibodies that targets different parts of the spike protein. Some antibodies will knockout the function of the spike protein and thereby neutralize the virus. While some will bind to the NTD segment of the spike protein and help the virus enter the cell, making the virus more infectious.
If you are lucky, your immune system develops more virus neutralizing antibodies than virus enhancing antibodies and you will probably have mild covid19. If you are unlucky and your immune system makes more infectivity enhancing antibodies, you will probably have a bad time.
This situation where antibodies can enhance the infectivity of the virus is called Antibody Dependent Enhancement (ADE). ADE is why on the second time you get infected by the dengue virus, you have a higher chance of developing the more severe haemorrhagic dengue fever.
Does this impact the current vaccines?
All three vaccines by Pfizer, Moderna and AstraZeneca that have been granted emergency use authorization retain the infectivity enhancing site on the NTD segment. This means exposure to these vaccines will result in the immune system developing some infectivity enhancing antibodies.
However there are vaccines still under development that target parts of
the spike protein, specifically the RDB tsegment. Most are research
groups inChina although BioNTech is also in that race. Thankfully nobody
has targeted the NTD segment for a vaccine target, eventhough the
region is very immunogenic. That would have made a disasterous vaccine.
What can we expect?
The proper scientific answer; We don’t know. More experiments need to be done to determine the severity of ADE associated with the three vaccine currently in use. The completion of the phase III trial will answer this question. The completion dates for the phase III trials from Pfizer is September 2021, Modena in October 2022 and AstraZeneca in February 2023.
The speculative coffee table answer; Since these is some level of ADE associated with whole spike protein, we should expect to see odd things occurring. For example, we will continue to observe severe cases of Covid19 despite immunization and a robust immune response became some people by chance will produce more bad virus enhancing antibodies than good neutralizing antibodies. This will be on top of cases when the vaccine fails and does not trigger an immune response.
Repeated infection are possible and subsequent infections are not necessarily milder and can be more severe. It will all depends on the pool of reactivated memory B cells that produces the ratio of good neutralize antibodies to bad infectivity enhancing antibodies. However given that over production of bad enhancing antibodies may be lethal, you won’t expect a person to be re-infected too many times.
Other oddities of SARS-Cov2 that maybe linked to ADE activity are incidence of persistence infection observed in a few covid 19 patients..where a person remains infected for over 60 days without clearing the virus.
What to do?
- Do more research.
We obviously want to know if there is more than one infectivity enhancing site on the spike protein. Liu et al, had six patient derived enhancing antibodies and they all bound to the same region. The numbers are small but it is hopeful that this one site is the most immunogenic and thus the only region that needs to be removed..
- Fix the vaccine.
In an ideal world, Liu et al study should be immediately rechecked. And if validated, vaccine developers would immediately create a new version of the vaccine and this time with a spike protein that lacked the NTD segment. Without the NTD, no infectivity enhancing antibodies would be developed by the immune system, thus making the vaccine safer and efficient. The efficacy of the new vaccine would need to be reevaluate as removal of the NTD segment could alter the shape of the pre-fusion spike protein and thus effect the efficacy of the vaccine.
Unfortunately we live in a non-ideal world, where everything doesn’t always go to plan. For nations that can afford the time, like Japan, China or South Korea, they should explore redesigning the Spike protein target to remove the infectivity enhancement site. But for the UK… where deaths are mounting from the new super spreader B117 strain.. they may have to roll out the original vaccine while testing the new vaccine. Sometimes all we can do is take the hit and build a better vaccine for those that come after us.
Also one Mystery solved (Maybe)!
This discovery of an infectivity enhancement site on the SARS-Cov2
spike protein, and subsequent viral enhancing antibodies is a possible
solution to the mystery of why convalescent plasma was such an
unreliable therapy (and why more antibodies wasn’t always better). Not
all the antibodies in that plasma was helpful. While some antibodies did
fight and neutralized the virus, other antibodies made the infection
worse by helping the virus gain entry into the host cell. Different
batches of convalescent plasma would have different ratios of good and
bad antibodies, with some having more good antibodies and other batches
less.
https://klse.i3investor.com/blogs/Pblue/2021-01-01-story-h1538489694-Top_Glove_Discovery_of_an_infectivity_enhancing_site_on_the_SARS_Cov2_s.jsp
